
Why Test for Genetic Markers? Enhancing Patient Safety Using Genetics
Consider the Drug Optimization Advantages of ChemaTox
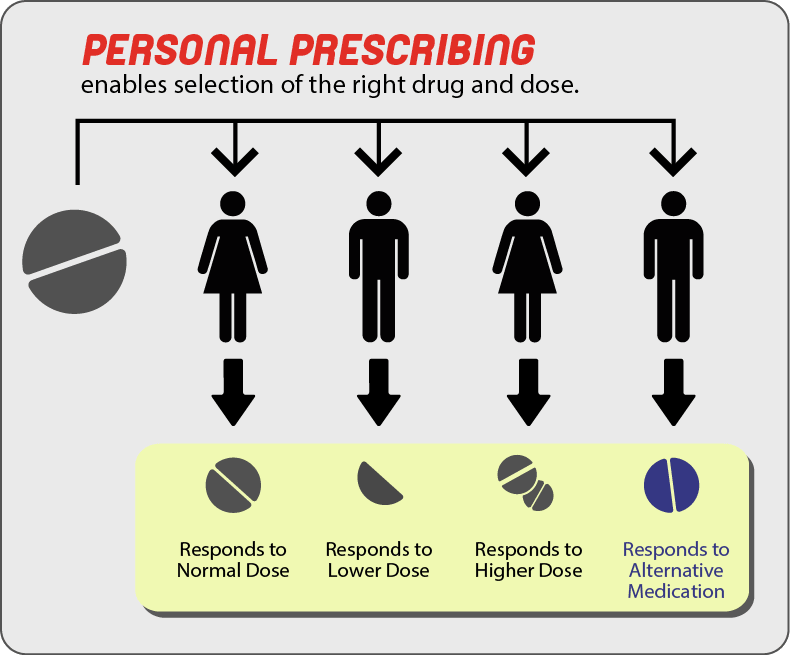
- Personalize treatment with better initial dosing
- Minimize side effects
- Reduce adverse drug events and treatment failures
- Improve patient care, reduce costs
- Enhance outcomes with better drug efficiency
The benefits are clear: Safer, more efficient and effective care + FDA requirements
Perhaps the most compelling argument for genetic testing for the purpose of patient care comes from the FDA itself in the requirement of pharmaceutical companies to include CYP450 metabolic status in labeling of certain drugs.(9,10) The information described in labeling plays an important role when identifying factors to avoid adverse effects, understand drug efficacy, and optimize drug dose. Having the ability to determine how a patient responds to drug therapies benefits the physician, the patient, and helps keep health care costs lower by avoiding the “trial and error” method of drug dosing.
Reducing Patient Side-Effects
Every time you turn on the television or radio you might hear ads for the latest drug therapy. Each ad is followed by a person speed reading through a list of possible side effects; anti-depressants, beta-blockers, statins, and many other common drugs all run the risk of severe side effects. Pharmacogenetic testing can help mitigate the risk of patients experiencing these side effects.
A group of liver enzymes known as the Cytochrome P450 group (CYP) is responsible for the metabolism of a large percentage of these drugs, and a person's genes play a very large role in how these drugs are metabolized.(4,6) Individuals with one or more inactive alleles of a gene are classified as poor or intermediate metabolizers. Conversely individuals with multiple copies or increased metabolic status due to mutations are classified as ultra-rapid metabolizers. The consequences of metabolic status depends on the drug prescribed, but in both cases the outcomes could be devastating.(4,8) Scientific literature has clear examples of patients suffering severe side effects, inefficacy, and even death due to their genetic make-up.
Opioid analgesics prescribed for mild to moderate pain relief include codeine, hydrocodone, oxycodone, and tramadol. The analgesic properties of these pro-drugs come from their conversion into their active metabolites by CYP2D6. Genetic variations in the CYP2D6 enzyme has been associated with deaths in children prescribed opioid medications undergoing routine tonsillectomy. Ultrarapid metabolizers of this enzyme can result in life-threatening adverse reactions in young children, particularly those with a history of sleep apnea.(1)
Moreover, understanding the genotype of a patient in relation to co-administration of drugs is imperative. Many drugs act as inhibitors or inducers of CYP enzymes which can affect the metabolic status of the patient.(9) Further, determining the genotype of a patient within in the context of family can have implications for other family members.
Tramadol is a synthetic opioid with low potential of respiratory depression and development of tolerance, and is often prescribed for general and post-operative pain relief.(5) When a 22-year-old female patient was admitted to an ICU in refractory cardiac arrest, blood analysis revealed high concentrations of tramadol and its metabolite O-desmethyltramadol. The patient was genotyped for CYP2D6 and it was found that she was heterozygous for a duplicated wild-type allele resulting in the ultrarapid metabolism of drugs. These findings were confirmed by the calculation of the tramadol/metabolite ratio. Proper dosing of tramadol based on her ultrarapid metabolic status may have prevented the incident.(3)
In fact it has been shown that metabolizer dependent response is not unique to a few individuals; one study involving 174 patients with various genotypes considered the concentrations of Tramadol and it's metabolite o-desmethyltramadol in relation to CYP2D6 metabolizer status (PM, IM, EM, UM) and found that concentrations of the metabolite depended on metabolic status. Metabolite concentrations increased from PM, IM, EM, and UM in a predictable, incremental way with PM's having the lowest concentrations of metabolites and UMs having the highest, showing a strong link between genetics and predictable outcome of drug therapy.(6) In another study involving 300 post-operative patients it was found that those in the PM group required higher doses with more frequent “rescue” doses of Tramadol than those in the EM group to maintain effective therapy.(5)
Tramadol and Opioids aren't the only drugs whose efficacy and side effects might depend on the patient's genotype. Literature has clearly shown that poor metabolizers are at increased risk of suffering adverse side effects and even suicide from many drugs including tricyclic antidepressants (TCA), selective serotonin re-uptake inhibitors, b-blockers, warfarin, and antipsychotics.(11,12,13,14) Moreover, co-administration of inhibitory drugs with substrates combined with genotype and copy number variants further complicates the ability to ensure positive outcomes.(12,15)
References
1) Sadhasivan S., Myer CM 3rd. Preventing opioid-related deaths in children undergoing surgery. Pain Med. 2012 Jul;13(7):982-3; author reply 984. doi: 10.1111/j.1526-4637.2012.01419.x. Epub 2012 Jun 13.
2) Madadi P, Hildebrandt D, Gong IY, Schwarz UI, Ciszkowski C, Ross CJ, Sistonen J, Carleton BC, Hayden MR, Lauwers AE, Koren G. Fatal hydrocodone overdose in a child: pharmacogenetics and drug interactions. Pediatrics. 2010 Oct;126(4):e986-9. doi: 10.1542/peds.2009-1907. Epub 2010 Sep 13.
3) Elkalioubie A, Allorge D, Robriquet L, Wiart JF, Garat A, Broly F, Fourrier F. Near-fatal tramadol cardiotoxicity in a CYP2D6 ultrarapid metabolizer. Eur J Clin Parmacol (2011) 67:855-858 DOT 10.1007/s00228-011-1080-x
4) Cohen M, Sadhasivam S, Vinks AA. Pharmacogenetics in perioperative medicine. Wolters Kluwer Health/Lippincott Williams & Wilkins. Vol 25, Num 4, August 2012
5) Stamer UM, Lehnen K, Hothker F, Bayerer B, Wolf, S, Hoeft A, Stuber F. Impact of CYP2D6 genotype on postoperative tramadol analgesia. Pain (2003) 231-238
6) Stamer UM, Musshoff F, Kobilay M, Madea B, Hoeft A, Stuber F. Concentrations of Tramadol and O-desmethyltramadol Enantiomers in CYP2D6 Genotypes. Clinical Pharmacology and Therapeutics. Volume 82, number 1, July 2007.
7) Van Driest SL, McGregor TL. Pharmacogenetics in clinical pediatrics: challenges and strategies. Per Med. Sep 2013; 10(7): 10.2217/pme.13.70.
8) Drögemöller BI, Wright GE, Warnich L. Considerations for rare variants in drug metabolism genes and the clinical implications. Expert Opin Drug Metab Toxicol. 2014 Jun;10(6):873-84. doi: 10.1517/17425255.2014.903239. Epub 2014 Mar 28.
10) http://www.fda.gov/drugs/scienceresearch/researchareas/pharmacogenetics/ucm083378.htm
11) Zackrisson, A.L., Lindblom, B. & Ahlner, J. High frequency of occurrence of CYP2D6 gene duplication/multiduplication indicating ultrarapid metabolism among suicide cases. Clin. Pharmacol. Ther. 88, 354–359 (2010).
12) Hiemke C, and Hartter S. Pharmacokinetics of Selective Serotonin Reuptake Inhibitors. Science Direct, 2000. Web. 13 May 2014.
13) Nagele P, Liggett SB. Genetic variation, β-blockers, and perioperative myocardial infarction. Anesthesiology. 2011 Dec;115(6):1316-27. doi: 10.1097/ALN.0b013e3182315eb2.
14) Wang D, Chen H, Momary KM, Cavallari LH, Johnson JA, Sadée W. Regulatory polymorphism in vitamin K epoxide reductase complex subunit 1 (VKORC1) affects gene expression and warfarin dose requirement. Blood. 2008 Aug 15;112(4):1013-21. doi: 10.1182/blood-2008-03-144899. Epub 2008 Jun 3.
15) Preskom SH, Alderman J, Chung M, Harrison W, Messig M, Harris S. Pharmacokinetics of desipramine coadministered with sertraline or fluoxetine. J Clin Psychoparmacol. 1994 Apr;14(2):90-8.